Fact-checked by
Fact-checked by There are several types of myasthenia gravis (MG), an autoimmune disease that affects communication between nerves and muscles.
MG occurs when the immune system mistakenly targets proteins that help nerves send signals to muscles. All main forms of the disease lead to characteristic symptoms of muscle weakness and fatigue, but they differ in which muscles are affected.
Beyond the primary MG disease classifications, there are also several MG clinical subtypes based on factors such as disease-causing antibodies, thymus gland involvement, and age of onset. Doctors use these classifications to help determine the best treatment and care plan.
Primary types
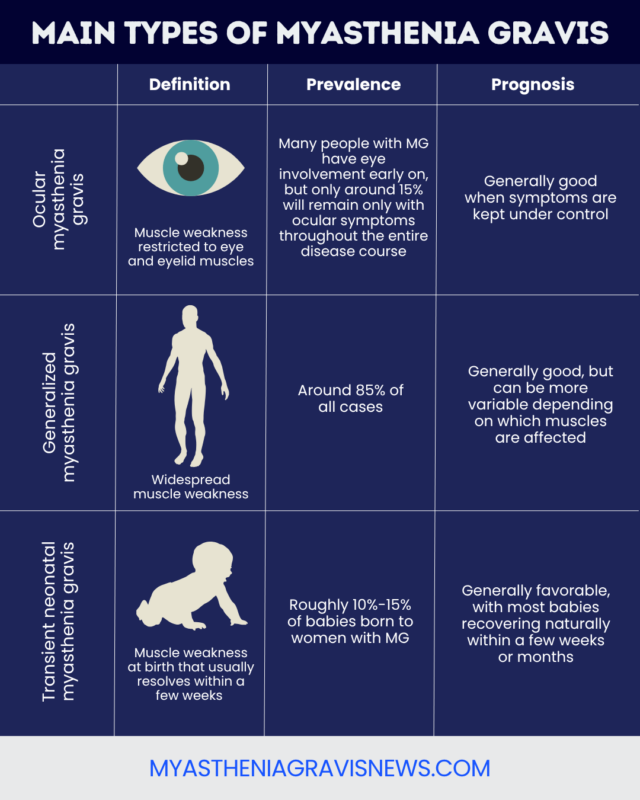
There are three main types of MG:
Ocular MG affects only the muscles around the eyes, while generalized MG also affects muscles elsewhere in the body. Transient neonatal MG is a temporary condition that develops in some infants whose biological mothers have MG.
A rare group of genetic conditions called congenital myasthenic syndromes (CMS) can cause symptoms similar to MG. However, CMS is not a type of MG and has different causes and treatments.
Ocular MG
In ocular MG, weakness is limited to the muscles that control the eyes and eyelids. Common symptoms include:
- droopy eyelids (ptosis)
- double vision (diplopia)
While many people with MG have some eye involvement early on, only around 15% of people with MG have purely ocular MG throughout the entire disease course.
Some people who start with eye weakness later develop weakness in other muscles and convert from ocular MG to generalized MG. The estimated ocular-to-generalized MG conversion rate varies across studies, from around 20% to 60%, with conversion typically occurring within two years of ocular symptom onset.
With treatment, ocular MG typically has a good prognosis, and life expectancy is generally normal.
Generalized MG
Generalized MG, or gMG, causes widespread muscle weakness and fatigue that is not limited to the eye muscles. It is estimated that around 85% of people with MG have gMG. Some people with gMG initially have generalized symptoms, while others start with ocular weakness and later experience MG symptom progression.
gMG can also affect various muscle groups, leading to clusters of symptoms:
- face and throat, or bulbar, muscles: difficulty speaking, swallowing, chewing, and controlling facial expressions
- neck muscles: difficulty holding up the head
- limb muscles: changes in walking patterns and movement difficulties
- respiratory muscles: shortness of breath and other breathing difficulties
The prognosis for gMG is also generally good, and many people have a relatively normal life expectancy. However, people with gMG have an increased risk of certain life-threatening complications, depending on which muscles are affected.
About 15% to 20% of people with gMG experience a myasthenic crisis at some point. This life-threatening complication occurs when the breathing muscles are severely affected. It often occurs during the first few years of the disease course.
Transient neonatal MG
Transient neonatal MG is a rare type of the disease that affects about 10% to 15% of infants born to mothers with MG. It occurs when the self-reactive antibodies that drive MG-related autoimmune attacks pass from the mother to the fetus during pregnancy.

Living with MG
Essential Life Hacks for Myasthenia Gravis


Living with MG
Navigating Mental Health with Myasthenia Gravis
Symptoms are usually apparent within hours to days after birth and may include:
- difficulty suckling or swallowing
- difficulty breathing
- generalized weakness
- weak cry
These symptoms are temporary and resolve within two months of birth in 90% of cases. Recovery occurs as the baby’s own antibodies replace those passed from the mother.
Doctors can’t reliably predict which babies will be born with the condition, and no known treatments effectively prevent mothers from passing on their self-reactive antibodies.
Classification by serotype
People with MG may also be grouped by their serotype, or the type of self-reactive antibodies found in their blood.
MG is caused by self-reactive antibodies that target proteins important for nerve-muscle communication. Several types of antibodies are linked to the disease, and most people with MG test positive for one of them. In a minority of people with MG, no known disease-causing antibody is detected.
Seropositive MG
Seropositive MG refers to people with detectable levels of known disease-causing antibodies. The most common antibodies target one of three proteins:
- acetylcholine receptor (AChR)
- muscle-specific kinase (MuSK)
- low-density lipoprotein receptor-related protein 4 (LRP4)
AChR-targeting antibodies are the most common, occurring in about 80% to 85% of people with gMG and about half of those with ocular MG. About 5% to 8% of people with MG have MuSK-targeting antibodies.
When comparing AChR versus MuSK antibody types, MuSK-positive MG is often associated with more severe symptoms and greater involvement of bulbar muscles. There’s no way to exactly predict myasthenic crisis risk by type, but people with MuSK antibodies may be more likely to experience respiratory complications.
LRP4 antibodies are a more recent discovery and may be associated with milder symptoms.
Seronegative and double-seronegative MG
In seronegative MG, blood tests don’t detect known disease-causing antibodies. This is sometimes referred to as double-seronegative MG when patients test negative for antibodies that target both AChR and MuSK.
This terminology predates the availability of tests for LRP4-targeting antibodies. Some of the approximately 10% of people with MG historically classified as double-seronegative may in fact have LRP4 or other antibodies.
Age-related subtypes
While MG can occur at any age, it is most commonly diagnosed in adult women younger than 40 and in men older than 60. Sometimes, the disease is classified based on when symptoms first emerge:
- early-onset MG: starts in adulthood, but before age 50
- late-onset MG: starts after age 50
- juvenile MG: starts during childhood or adolescence
There are several differences between early-onset and late-onset MG. Early-onset MG more commonly affects women, while late-onset MG may affect men at slightly higher rates. Additionally, people who develop the disease earlier are more likely to have generalized muscle weakness among their early symptoms.
A juvenile MG diagnosis, though overall rare, is most common in teenage girls and can cause symptoms similar to those of adult MG.
Classification by thymus involvement
Abnormalities in the thymus gland, an immune organ in the chest, may contribute to the production of AChR-targeting antibodies in MG. About 70% of people with MG have an enlarged thymus, and about 10% to 20% have a type of thymus tumor called thymoma.
Thymoma-associated MG often causes moderate-to-severe symptoms that affect multiple muscle groups. A surgical procedure to remove the thymus, called a thymectomy, can help ease symptoms for some people with MG.
MGFA clinical classification
The Myasthenia Gravis Foundation of America (MGFA) has a system for rating MG severity. The MGFA clinical classification system groups people with MG into five classes based on the degree and location of muscle weakness.
| MGFA Class | Clinical Characteristics |
|---|---|
| I | Any ocular muscle weakness, but no other muscle weakness |
| II | Mild weakness in non-ocular muscles, with or without ocular weakness |
| III | Moderate weakness in non-ocular muscles, with or without ocular weakness |
| IV | Severe weakness in non-ocular muscles, with or without ocular weakness |
| V | Requiring a tube inserted into the windpipe to help with breathing |
Within classes II, III, and IV, there are also subclasses that further specify which muscle groups are affected. Subclass A mostly involves muscle weakness in the limbs and trunk, while subclass B mainly involves bulbar and respiratory muscles.
Myasthenia Gravis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.