
 Fact-checked by
Fact-checked by 
Myasthenia gravis treatment
There is no cure for the neuromuscular condition myasthenia gravis (MG), but a number of different treatment approaches are available to help manage its symptoms. Treatments, which may include medications, surgery, or other procedures, generally aim to either suppress the harmful effects of the immune system on the body, or to restore nerve-muscle communication.
MG is caused by the immune system’s misdirected attack against proteins required for communication between nerves and muscles, which leads to insufficient muscle contraction and the hallmark disease symptoms of muscle weakness and fatigue.
The particular treatments that might help each individual patient will depend on a number of factors, including symptom severity, MG type, and cause. Some myasthenia gravis patients also may go into spontaneous remission in the absence of treatment.
Medications
There are a number of approved medications that can be prescribed after receiving a MG diagnosis. Each medication works via a different mechanism to ease symptoms of muscle weakness and fatigue. Some myasthenia gravis medications are given orally, whereas others require injections or infusions. Not all medications will work for every patient.
Anticholinesterases
Anticholinesterases, or acetylcholinesterase inhibitors, are often a first-line treatment for MG. They are designed to prevent the destruction of the signaling molecule acetylcholine — which serves as a chemical messenger between nerve and muscle cells to coordinate muscle contraction — and boost its effects.
These medicines work by blocking the activity of acetylcholinesterase, the enzyme that normally breaks down acetylcholine. Anticholinesterases may be given orally, as intravenous (into-the-vein) infusions, or by intramuscular (into-the-muscle) injections.
Acetylcholinesterase inhibitors that may be used for treating MG include:
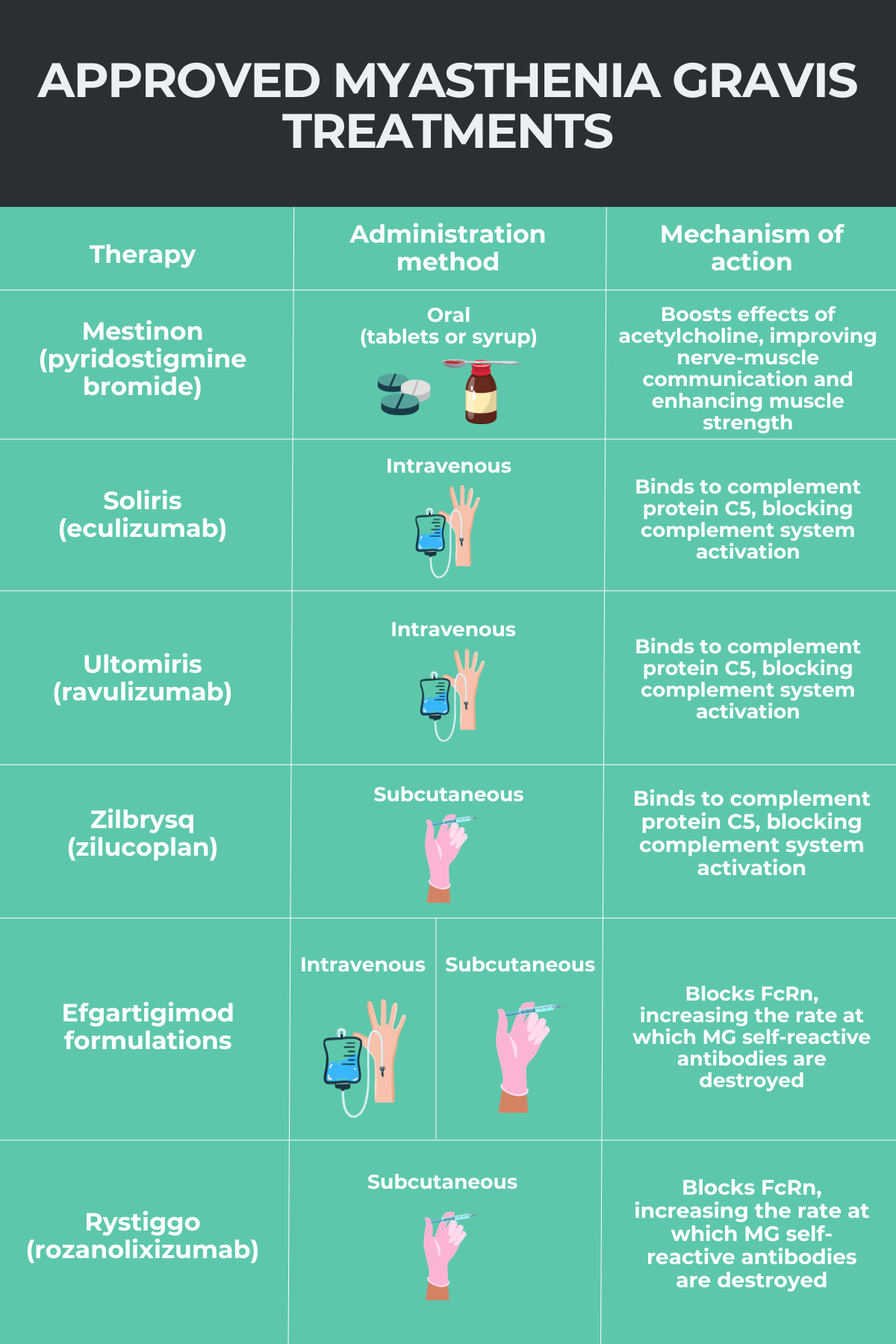
- Mestinon (pyridostigmine bromide), available as a syrup, conventional tablets, or extended-release tablets, and the most commonly used of this class of medications
- injectable versions of pyridostigmine or neostigmine, given when patients cannot take oral medications, and typically used in more severe cases, such as in the event of a myasthenic crisis.
Generics of oral Mestinon are also available for MG patients.
Acetylcholine receptors (AChRs) — the receptors on muscle cells through which acetylcholine exerts its effects — are targeted and attacked by the immune system in most patients with MG. These medications do not directly affect this immune response, but rather work to counteract its effects by increasing acetylcholine levels. Thus, while anticholinesterases do not address the underlying causes of myasthenia gravis, they can effectively enhance muscle strength.
Complement inhibitors
The immune system’s complement signaling cascade is thought to contribute to the autoimmune attacks that characterize MG, particularly when antibodies against AChRs are present.
Complement inhibitor therapies work to suppress the activation of the complement system, thereby helping to control the immune activity that leads to muscle weakness for people with generalized myasthenia gravis (gMG) who are positive for anti-AChR antibodies.
There are three approved complement inhibitor therapies for MG, all of which target the C5 protein, a component of the complement cascade. These are Soliris (eculizumab), Ultomiris (ravulizumab-cwvz), and Zilbrysq (zilucoplan).
Soliris and Ultomiris are both given via into-the-vein infusions. Ultomiris is designed to allow for a less frequent dosing schedule than Soliris, its predecessor. Zilbrysq is given once daily, via subcutaneous (under-the-skin) injections. Unlike Soliris and Ultomiris, with appropriate training, Zilbrysq can be given by caregivers or self-administered by patients.
All three complement inhibitors are currently approved in the U.S. to treat gMG patients who are positive for anti-AChR antibodies. Soliris is approved for children and adults, while Ultomiris and Zilbrysq are only approved for adult patients.
More like this...


Living with MG
Navigating Mental Health with Myasthenia Gravis
FcRn blockers
The self-reactive antibodies that drive MG belong to an antibody family called immunoglobulin G, or IgG. The neonatal Fc receptor (FcRn) is a protein that helps to stabilize IgG antibodies circulating in the bloodstream.
FcRn blockers work to inhibit that protein, thereby increasing the rate at which these self-reactive antibodies are broken down, and easing disease symptoms.
To date, several FcRn blockers have been approved to treat MG. These include Vyvgart and Vyvgart Hytrulo (efgartigimod formulations), both of which have been approved to treat gMG in all adults. Vyvgart is given via an infusion directly into the bloodstream, while Vyvgart Hytrulo is administered by a subcutaneous injection.
Rystiggo (rozanolixizumab-noli) and Imaavy (nipocalimab-aahu), two other FcRn blockers, have also been approved to treat gMG patients who are positive for antibodies targeting AChR or muscle-specific kinase (MuSK). Rystiggo has only been cleared for adults, while Imaavy is authorized for use in adults and adolescents ages 12 and older.
A number of other experimental FcRn blockers, including batoclimab, are under investigation as possible treatments for MG.
B-cell-depleting therapies
B-cells are the immune cells mainly responsible for producing antibodies, including the harmful ones that drive MG. B-cell-depleting therapies, which work by lowering the number of B-cells, can help reduce the levels of MG-causing antibodies, thereby easing disease activity and symptoms.
Uplizna (inebilizumab-cdon) is the first and only B-cell-depleting therapy to be approved for MG. It’s specifically indicated for the treatment of adults with gMG who are positive for anti-AChR or anti-MuSK antibodies. The therapy is given via into-the-vein infusions, which are given every six months after two loading doses.
Corticosteroids
Corticosteroids, a type of anti-inflammatory drug, are also widely used to treat MG symptoms. They broadly work by suppressing the activity of the immune system. These treatments are sometimes initiated after others, such as acetylcholinesterase inhibitors, have failed to control MG symptoms.
Prednisone is the most common corticosteroid used to treat MG. Other steroids that may be used for MG include:
- prednisolone
- dexamethasone
- hydrocortisone
- triamcinolone.
Because long-term use of corticosteroids is associated with significant side effects, these medications often are used in combination with other treatments that aim to be steroid sparing. That allows for a lower dose of steroids to be used or for these medicines to be stopped altogether.
Immunosuppressants
A number of nonsteroidal general immunosuppressants also may be used to control immune activity in MG. As with corticosteroids, these medications don’t specifically target known MG disease mechanisms, but rather serve to broadly suppress the immune system via a range of different mechanisms.
General immunosuppressants used to treat MG include:
- azathioprine, sold as Imuran, among other brand names
- mycophenolate mofetil, sold as CellCept
- cyclophosphamide, sold as Cytoxan, among other brand names
- cyclosporine, sold as Gengraf, among other brand names
- methotrexate, sold as Trexall, among other brand names
- tacrolimus, sold as Prograf, among other brand names.
Plasmapheresis
Also known as plasma exchange, plasmapheresis is a type of blood-filtering treatment for autoimmune diseases.
In this procedure, blood is drawn from a patient and its liquid component — plasma, which contains the self-reactive antibodies driving MG — is filtered out. The plasma then is replaced with a fluid that does not contain antibodies and infused back into the patient.
Plasma exchange is thought to reduce the levels of the self-reactive antibodies that cause MG, helping to ease its symptoms. However, the process does not distinguish between disease-driving and regular infection-fighting antibodies, and thus can lead to immune suppression.
The process of plasmapheresis usually takes a few hours, and can be completed in the hospital or in an outpatient setting. Most patients recover quickly after the procedure, but may feel tired or lightheaded for a while afterward.
Plasma exchange does not stop the body from producing more self-reactive antibodies. Thus, while its effects are fast, they also are temporary. The procedure also is time-consuming and can be costly, so it’s not typically used as a routine therapy. Instead, it is more commonly used for patients with severe symptoms or for those requiring emergency interventions, such as during a myasthenic crisis.
Intravenous immunoglobulin infusion
Intravenous immunoglobulin (IVIG) infusions are another way of combating the harmful, self-reactive antibodies that drive MG. With this approach, pooled immunoglobulins — consisting mostly of IgG antibodies — obtained from healthy donors are infused into a patient’s bloodstream.
While its mechanisms are not entirely understood, it is thought that the donor IgGs lead to temporary immune system modifications that can help to neutralize and promote the elimination of self-reactive antibodies, ultimately damping down the autoimmune process.
The treatment is infused slowly over a period of several hours, and may involve a series of infusions over a few days. It’s usually well tolerated, but patients may experience fatigue, fever, or nausea for about a day after an infusion.
As with plasmapheresis, this treatment is time-consuming and expensive. It’s generally reserved for patients with severe symptoms, such as those experiencing a myasthenic crisis, those who are not responding to other therapies, or people who are about to undergo surgery.
Thymectomy
The thymus gland, a component of the immune system located under the breast bone, is responsible for the production and maturation of certain immune cells. Abnormalities in this gland are thought to contribute to the production of the self-reactive antibodies that drive MG.
Some patients have a thymoma, or a tumor in the thymus gland, while others have thymic hyperplasia, or an enlarged gland.
Surgery to remove the thymus, called a thymectomy, may be recommended for some MG patients, especially those with a thymoma, or individuals younger than age 60 with mild to moderate generalized muscle weakness.
There are a number of different approaches a doctor might take to perform the surgery, but the procedure today is typically conducted in a minimally invasive manner: A surgeon makes a small incision in the patient’s chest and uses a tiny camera to assist in removing the thymus gland.
Although its effects are not immediate, a thymectomy can ease muscle weakness, lower the doses of steroids or other medications used, and reduce the risk of severe symptoms requiring hospitalization in MG patients. About 70% of patients achieve complete remission or a significant reduction in medication usage within a year of undergoing surgery.
Avoiding triggers
A number of different factors can trigger the onset or worsening of myasthenia gravis symptoms. Avoiding known disease triggers also may be a way of preventing or easing symptoms of MG.
Common myasthenia gravis triggers include:
- stress and anxiety
- fatigue and lack of sleep
- infections, illness, and pain
- hormonal changes, including those occurring during pregnancy or menstruation
- extreme temperatures
- certain medications or changes in medications.
Maintaining a healthy lifestyle, including a proper diet, staying well rested, exercising, and avoiding stress can help to prevent symptoms from occurring as frequently.
Emergency treatment
When MG symptoms suddenly worsen, patients can develop severe muscle weakness resulting in life-threatening shortness of breath, called a myasthenic crisis. These crises require hospitalization and emergency treatment.
During such events, patients usually require the temporary use of a ventilator, oxygen mask, or other breathing support in the hospital. Therapies like plasmapheresis and IVIG also are commonly used to rapidly control MG symptoms and stabilize a person’s breathing.
Support groups
Living with myasthenia gravis can take a toll on a person’s mental and emotional health, particularly if a patient’s participation in daily activities becomes limited due to muscle weakness. Managing these changes can be an important part of a person’s myasthenia gravis treatment plan.
Individuals facing depression, anxiety, or stress due to MG should speak with their healthcare team about appropriate treatments, which may include medications, therapy, exercise, rest, or other lifestyle changes.
Local support groups also are a helpful way for patients to connect with others in the MG community. The Myasthenia Gravis Foundation of America has multiple myasthenia gravis support groups across the U.S., which provide an opportunity for patients to share their stories and learn from others. Patients also can gain access to resources and educational programs, and participate in recreational activities through these groups.
The Myasthenia Gravis News Forums also offer platforms for patients and caregivers to connect with one another about topics related to living with myasthenia gravis, such as relationships, maintaining a healthy lifestyle, mental health support, and others. There also are various columns in which patients discuss their own experiences.
Myasthenia Gravis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about myasthenia gravis treatment
Category:
Treatment
The best treatment for myasthenia gravis will vary depending on a person’s symptoms and their severity, the cause and type of the disease, and other health factors. Treatment regimens may change over time as a person’s disease evolves. Patients should work with their individual healthcare teams to decide on an appropriate course of treatment in their particular case.
Category:
Treatment
Whether myasthenia gravis treatments are covered by a person’s insurance — and to what degree they’re covered — will depend on each person’s particular insurer and plan. Patients are advised to speak with their healthcare team and insurance company when starting a new treatment to understand their individual coverage. Some companies marketing myasthenia gravis medications also offer support in navigating the insurance process and accessing financial assistance programs.
Category:
Treatment
There is no cure for myasthenia gravis, but there are several treatments, including medications, plasmapheresis (plasma exchange), and surgery, that can help ease its symptoms. Many of these treatments work to either suppress the activity of the immune system or improve nerve-muscle communication to alleviate symptoms of muscle weakness and fatigue.
Category:
Treatment
Although they work through different mechanisms, myasthenia gravis treatments are intended to ease or prevent the symptoms of muscle weakness and fatigue that characterize the neuromuscular disease. These treatments usually do so by either suppressing the immune system or enhancing nerve-muscle communication.
Category:
Treatment
A number of medications exist that can help manage myasthenia gravis symptoms. Medications for myasthenia gravis, or MG for short, can be divided into multiple groups depending on their mechanism of action, to include anticholinesterases, complement system inhibitors, FcRn blockers, corticosteroids, or non-steroidal immunosuppressants. However, none of these therapies provides a definite cure for the condition.
Related Articles
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion