Early-onset vs. late-onset myasthenia gravis
 Fact-checked by
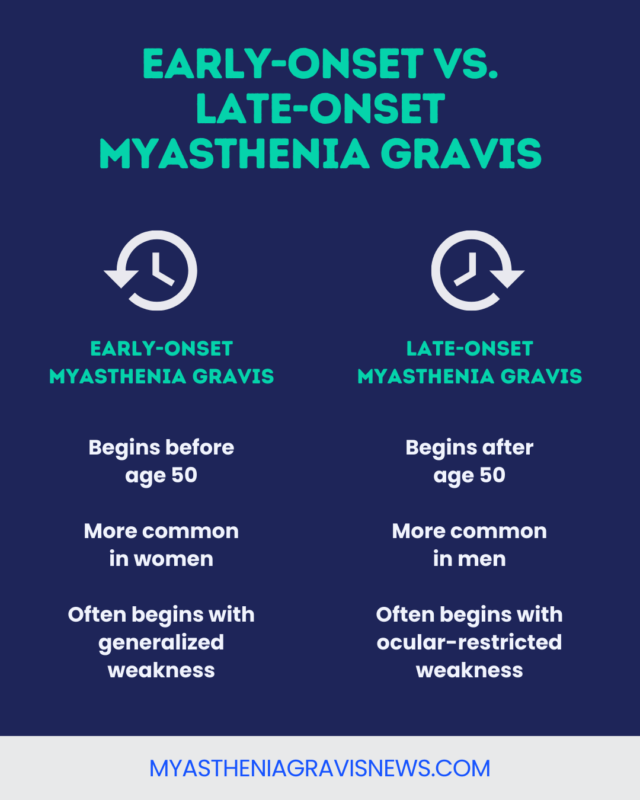
Fact-checked by Myasthenia gravis (MG) is an autoimmune neuromuscular disease that affects people at different life stages. Whether someone has early-onset myasthenia gravis (EOMG) or late-onset myasthenia gravis (LOMG) — distinguished by whether symptoms begin before or after age 50 — may have implications for diagnosis and treatment.
MG is caused by self-reactive antibodies that direct immune attacks against acetylcholine receptors (AChRs) or other proteins that help nerves and muscles communicate. This leads to characteristic MG symptoms of muscle weakness and fatigue.
The rare disease can be diagnosed in childhood (juvenile MG) or adulthood. For people with adult-onset MG, the disease may be categorized as EOMG or LOMG. Some people may be considered to have very late-onset MG if their symptoms emerge at age 65 or older. EOMG is more often diagnosed in women, while LOMG is slightly more common in men.
How symptoms look at different age onsets
There are two main types of MG that affect adults: ocular MG, in which muscle weakness is restricted to the eyes and eyelids, and generalized MG, where such weakness is more widespread. Either disease type can affect people at any age. However, certain symptom patterns are more common in EOMG or LOMG:
- At disease onset, LOMG is more likely than EOMG to present with ocular-restricted disease, while EOMG is more likely to take a generalized course from onset.
- If LOMG does start with generalized weakness, it is more likely to be severe or life-threatening, with symptoms affecting the airways or other muscles in the face, mouth, and throat that are needed for swallowing and speaking (bulbar muscles).
- Among adults who initially have ocular symptoms, those with later-onset disease may be less likely to eventually progress to generalized weakness in MG.
Abnormalities in the thymus gland, an immune organ, can contribute to the development of MG at any age, but this is more common in people with EOMG. In particular, an enlarged thymus gland is much more strongly linked to EOMG, whereas data on thymus tumors (thymomas) are less clear.
EOMG is generally associated with fewer comorbidities — coexisting medical conditions including high blood pressure, high cholesterol, and diabetes — than LOMG.
| Early-onset MG | Late-onset MG |
|---|---|
| Often generalized at onset | Often ocular at onset, but generalized symptoms may be more severe if present |
| Thymus abnormalities are more common | Thymus abnormalities are less common |
| Typically fewer comorbidities | Typically more comorbidities |
People with LOMG may also experience more profound fatigue, although this symptom is common among all people with MG.
Diagnosis at different age onsets
Common diagnostic tests for MG are:
- physical and neurological examinations to identify muscle weakness
- the ice pack test to assess eyelid droopiness, a symptom of ocular MG
- blood tests to measure the levels of MG-causing antibodies
- repetitive nerve stimulation and electromyography to evaluate nerve-muscle communication
- imaging scans to identify thymus abnormalities
These tests help establish an MG diagnosis regardless of age, but some results may be more challenging to interpret in LOMG. For example:
- muscle weakness and other symptoms may be mistakenly attributed to aging or comorbidities
- natural age-related shrinking of the thymus can make it harder to distinguish MG-related changes
These complicating factors can lead to missed or delayed diagnoses, which are common in LOMG.
Treatment approaches
In general, all classes of approved MG treatments can be used in both EOMG and LOMG, with specific medication choices tailored to an individual’s disease severity, antibody status, and treatment tolerability. Treatments may include:
- Anticholinesterases: These therapies work to boost nerve-muscle communication and overcome the loss of AChRs.
- Complement inhibitors: These work to block an immune signaling pathway that contributes to MG.
- Neonatal Fc receptor (FcRn) blockers: Such therapies work to increase the rate at which disease-driving antibodies are broken down.
- B-cell depleting therapies: These work to lower the levels of immune cells that make disease-causing antibodies.
- Corticosteroids and other immunosuppressants: These medications help suppress the immune system to prevent its harmful attacks.
- Thymectomy: This involves the surgical removal of the thymus gland, a possible center of autoimmune activity.
There are, however, age-related considerations that may affect MG management decisions, including:
- Older people may have more comorbidities, and the medications used to treat them could potentially interact with MG therapies or worsen disease symptoms.
- Medication side effects, particularly infection risks with corticosteroids and other immunosuppressants, could have a greater impact on older people.
- A thymectomy for MG may be less effective in late-onset patients, and the surgical procedure may carry higher risks in this population; as such, the procedure is generally recommended for younger patients.
Long-term outlook
Some studies have shown that MG prognosis tends to be poorer in people who start experiencing symptoms later in life, with such patients being less likely to reach a state of low disease activity, or remission, although many do respond to treatment.
Other data suggest that with early intervention, most people with LOMG respond well to treatment, though individuals with EOMG tend to require more medications and are more likely to be resistant to treatment.
Quality of life may be poorer in late-onset populations and in older people living with MG of any type.
Regardless of the age of onset, people with MG should closely monitor their symptoms and report any changes to their doctors. Regular follow-up care is key to monitoring disease progression and treatment response.
Supportive and emotional care can help improve the quality of life for many people with MG and for those close to them. Joining patient or caregiver support groups for MG may provide a space to receive practical advice and management tips and to process emotions at any age.
Myasthenia Gravis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.