
Age Among Factors Affecting Survival in MG Patients with Thymoma Surgery
Written by |

Younger age, more advanced thymoma (tumors of the thymus) and cancer recurrence predict poorer survival in people with myasthenia gravis (MG) whose tumors are surgically removed, a large study from China reports.
Older age, in contrast, seems to protect against the likelihood of a tumor returning.
The study, “Surgical effect and prognostic factors of myasthenia gravis with thymomas,” was published in the journal Thoracic Cancer.
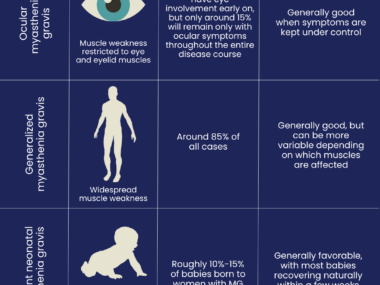
Estimates suggest that about 15% of MG patients develop thymomas. Surgery to remove these tumors — called thymectomy — is indicated for all MG patients independent of MG type and status. In an extended thymectomy, the entire thymus and the fat tissue located behind the mediastinum (the thoracic cavity midline) are removed.
Previous studies have investigated how different surgical approaches, including minimally invasive strategies, affect patient recovery and outcomes. However, few studies have looked into which factors influence survival of MG patients with thymoma.
Researchers in China investigated how different disease characteristics, surgery approaches and post-operative care might affect outcomes.
They analyzed data on 194 patients (median age, 49.9) with thymoma who underwent surgery at the Peking University People’s Hospital and Beijing Hospital between January 2010 and December 2018.
Before surgery, 157 patients were treated with pyridostigmine bromide (sold as Mestinon by Bausch Health; generic versions are also available), five with pyridostigmine bromide and the immunosuppressant Prograf (tacrolimus, by Astellas Pharma), and other five with intravenous (IV, into-the-vein) immunoglobulins (IVIG). The remaining 27 patients had mild symptoms and were not being treated.
Twenty-two patients had other autoimmune diseases besides MG, including thyroid diseases, skin-related conditions, ulcerative colitis, and other chronic inflammatory disorders.
Most patients (137) underwent video-assisted thoracoscopic surgery (VATS) thymectomy, a minimally invasive procedure that uses small incisions to insert a camera and instruments through the chest wall. Fifty-seven underwent transsternal thymectomy, an invasive procedure similar to open heart surgery.
Patients treated with VATS (mean age, 50.8) had shorter hospital stays and fewer complications, including lesser blood loss. They also had smaller tumors. Those in late tumor stages more often underwent transsternal surgery (mean age, 47.8).
After surgery, 77 patients were given radiotherapy, six chemotherapy, and three both.
Among the initial 194 patients, 170 were followed after surgery for a median of 45 months (almost four years). The median recurrence-free period was 39.5 months, and thymoma returned in 16 (9.4%) patients.
A majority — 81.9% — of patients were alive five years post-surgery. Fifteen died during follow-up: eight due to MG, five due to cancer’s recurrence, one to stroke (cerebral infarction), and one of unknown causes.
Further analysis indicated that age, the tumor’s stage under the Masaoka system (a common way of classifying thymomas), and cancer recurrence were independent predictors of overall survival.
Recurrence was more frequent in younger patients and those with more advanced tumors (Masaoka stages 3 and 4).
A post-operative myasthenic crisis (POMC) — a severe exacerbation of MG symptoms — was experienced by 20 patients in the first month after surgery. POMC incidence was significantly associated to the presence of bulbar symptoms (such as difficulty swallowing and slurred speech).
Researchers also evaluated the effectiveness of thymectomy in 162 patients. The overall effective rate was 84.5%. This rate accounts for cases with complete stable remission, pharmacological remission, minimal manifestations, and eased symptoms.
By the end of the second year after surgery, the cumulative complete stable remission rate was 19.3%, which increased to 44.1% by the fifth year. No rate differences were found between VATS and transsternal thymectomy, indicating that less invasive procedures can be similarly effective.
Overall, “extended thymectomy should be performed in patients with thymoma and MG. Age, Masaoka stage, and recurrence were prognostic factors for OS [overall survival],” the researchers wrote. In turn, having bulbar symptoms “was an independent risk factor for POMC.”
“The VATS procedure could achieve similar treatment effects of MG with thymoma,” the added.

Leave a comment
Fill in the required fields to post. Your email address will not be published.