
 Discussion
Discussion
Generalized myasthenia gravis
Last updated Nov. 3, 2025, by Lindsey Shapiro, PhD
 Fact-checked by Joana Carvalho, PhD
Fact-checked by Joana Carvalho, PhD
Generalized myasthenia gravis (gMG) is the most common and severe type of myasthenia gravis (MG), an autoimmune neuromuscular disorder that leads to muscle weakness and fatigue.
In contrast to ocular MG, where weakness is limited to the muscles controlling the eyes and eyelids, people with gMG may experience weakness in a broader range of muscles throughout the body. It is estimated that about 85% of people with MG have the generalized form of the disease.
There are treatments available to keep gMG symptoms under control, and while it can’t be cured, most people with gMG have a normal life expectancy with appropriate care.
What is generalized myasthenia gravis?
MG is an autoimmune condition in which the immune system erroneously produces self-reactive antibodies that lead to the destruction of proteins important for nerve-muscle communication. In about 85% of cases, these antibodies specifically target acetylcholine receptors (AChRs). A loss of signals that normally facilitate proper muscle contractions leads to chronic muscle weakness and fatigue.
gMG is a type of MG that normally emerges in adulthood and is characterized by muscle weakness that is not limited to a particular muscle group. It can involve any voluntary muscles, including those of the eyes, limbs, face, neck, and throat, as well as those needed for breathing. However, the specific muscles that are affected and the extent to which they are impacted is highly variable.
Other MG types are the eye-restricted ocular MG, as well as transient neonatal MG, a form of the condition that occurs in infants born to mothers with MG but is usually temporary. Another group of rare neuromuscular disorders, called congenital myasthenic syndromes, can have similar symptoms to gMG, but typically emerge in early childhood and are not autoimmune in nature.
Causes and risk factors
The exact cause of gMG is not known, but all evidence points toward immune dysregulation as a central aspect:
- Many people with gMG have abnormalities in the thymus gland, an important immune organ. This is thought to contribute to the production of self-reactive antibodies.
- gMG sometimes co-occurs with other autoimmune conditions, such as rheumatoid arthritis, lupus, or Hashimoto’s thyroiditis.
gMG is not considered to be an inherited condition, but in a small number of cases, patients have family members with gMG or other autoimmune conditions. Inherited variation in genes that influence immune function, such as the HLA genes, may play a role in such occurrences.
Generalized MG occurs in people of all races and ethnicities. The disease most commonly affects young women — those younger than 40 — and older men, specifically those older than 60.
Scientists have identified some risk factors that may make a person more likely to convert from the milder ocular MG to gMG. These include:
- older age at disease onset
- the presence of anti-AChR antibodies
- a thymus tumor, or thymoma
- abnormal findings on a repetitive nerve stimulation (RNS) test, which measures a muscle’s response to nerve stimulation
Symptoms of generalized myasthenia gravis
The hallmark symptom of MG is fluctuating muscle weakness that tends to worsen with physical activity and ease with rest.
Often, eye muscles are the first to be affected, leading to symptoms like eyelid droopiness, known as ptosis, and double vision, called diplopia. If symptoms stay that way, a person has ocular MG. But as many as 80% of people eventually develop problems in other muscle groups — usually within the first couple of years — and will be diagnosed with gMG.
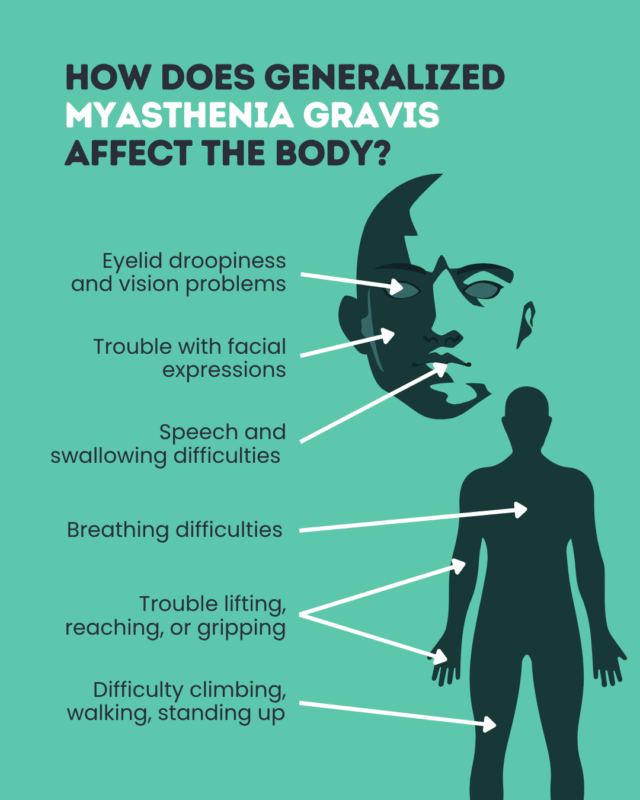
Beyond the eyes, muscle weakness in gMG can lead to:
- limb weakness, causing difficulty with daily activities like climbing stairs, lifting items, gripping things, or walking long distances
- facial muscle weakness, causing issues with speech and facial expressions
- throat and jaw weakness, which can cause difficulty chewing and swallowing
- shortness of breath, due to respiratory muscle weakness
About 15% of people with gMG have bulbar symptoms, or those associated with weakness in the head and neck, as their first symptoms.
Sudden and severe weakening of respiratory muscles can lead to a myasthenic crisis, which is life-threatening and requires emergency care.
Diagnosis
Reaching a gMG diagnosis may involve a series of diagnostic tests. These might include:
- a physical and neurological exam to evaluate muscle strength, reflexes, and symptom patterns
- an ice pack test, which looks for patterns of eye muscle weakness and recovery that are characteristic of MG
- blood tests to detect disease-causing antibodies
- RNS and electromyography, to measure the response of nerves and muscles to stimulation
- imaging tests, to identify thymus abnormalities and rule out other neurological diseases
These tests will help identify MG in general and rule out other conditions. Any patterns of weakness seen will also help determine if a person has gMG or ocular MG.
Treatment options
gMG can’t be cured, but there are a number of treatments that can help ease muscle weakness and keep the disease under control. gMG treatment often involves medications:
- Cholinesterase inhibitors such as Mestinon (pyridostigmine bromide), can be used to boost nerve-muscle communication.
- Complement inhibitors, including Soliris (eculizumab), Ultomiris (ravulizumab-cwvz), and Zilbrysq (zilucoplan), may inhibit an immune pathway implicated in gMG.
- FcRn blockers, including Vyvgart (efgartigimod alfa-fcab), Vyvgart Hytrulo (efgartigimod alfa and hyaluronidase-qvfc), Rystiggo (rozanolixizumab-noli), and Imaavy (nipocalimab-aahu), may lower the levels of disease-causing antibodies.
- Corticosteroids, such as prednisone, may suppress the immune system.
- Nonsteroidal immunosuppressants, like azathioprine, mycophenolate mofetil, cyclosporine, and others, can be used to suppress the immune system.
- B-cell depleting therapies, like rituximab, may lower levels of the immune cells that produce harmful antibodies.
All complement inhibitors, as well as Vyvgart/Vyvgart Hytrulo, are specifically approved for gMG patients with anti-AChR antibodies. Rystiggo and Imaavy can also be used in people with antibodies against the muscle-specific kinase, or MuSK, protein.
For people with involvement of the thymus gland, surgical removal of the thymus, called a thymectomy, may also be done.
In the case of a myasthenic crisis, emergency treatments may be used to quickly lower a person’s levels of self-reactive antibodies and ease symptoms. Such treatments include:
- plasmapheresis, or plasma exchange
- intravenous immunoglobulin therapy
Various experimental treatments are also being tested for gMG.
Managing daily life with gMG
Beyond MG medication, there are steps that can be taken in daily life to make living with gMG easier. These may include:
- creating a daily routine to work with fluctuating energy levels
- making dietary adjustments if chewing and swallowing are difficult
- taking part in physical therapy, to include moderate and appropriate exercises that boost muscle strength without worsening MG fatigue
- resting when feeling fatigued
- using assistive devices, like mobility aids, to conserve energy
- avoiding known symptom triggers, such as infections, heat, stress, or certain medications
- finding mental health support and coping strategies, such as counseling/therapy or support groups
Outlook and long-term management
The symptoms of gMG fluctuate over time, with periods where they are mild or absent — known as remission — interspersed with periods of symptom worsening, called flares or exacerbations. In some cases, a person in remission may be able to temporarily or permanently stop treatment.
There is no cure for gMG, but most people with the disease have a normal life expectancy. Regular monitoring and coordinated disease management with a multidisciplinary care team are key to ensuring the best possible outcomes.
gMG takes a physical and emotional toll. Beyond a healthcare team, it is important to build a strong support network, including:
- caregivers, family members, and friends
- patient and caregiver support groups
MG support and resources can be found in several places. Various advocacy organizations, including the Myasthenia Gravis Foundation of America, offer programs to link people with gMG to their peers. The forums of Myasthenia Gravis News also offer a way for people affected by gMG to connect.
Myasthenia Gravis News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion